


The Learning Triangle
- …
The Learning Triangle
- …
Primitive Reflexes
Primitive Reflexes are the first part of the brain to develop and should only remain active for the first few months of life. In typical development, these reflexes naturally inhibit in sequential order during the first year, and replacement reflexes, called postural reflexes, emerge. Postural reflexes are more mature patterns of response that control balance, coordination and sensory motor development.
Primitive reflexes naturally fade early in life, replaced by postural reflexes. Retained primitive reflexes may cause developmental delays, affecting various aspects like coordination, balance, sensory perception, and learning.
Retained primitive reflexes can lead to developmental delays related to disorders like ADHD, sensory processing disorder, autism, and learning disabilities. The persistence of primitive reflexes contribute to issues such as coordination, balance, sensory perceptions, fine motor skills, sleep, immunity, energy levels, impulse control, concentration and all levels of social, emotional, and intellectual learning.
Causes of Retained Primitive Reflexes
Retention of primitive reflexes can be caused by a variety of factors. The birth process is a key factor in the integration of these reflexes. Therefore a traumatic birth experience or birth by c-section may lead to retained reflexes. Additional causes can include: falls, traumas, lack of tummy time, delayed or skipped creeping or crawling, chronic ear infections, head trauma and vertebral subluxations.
Types of Primitive Reflexes
Moro Reflex
The Moro reflex acts as a baby’s primitive fight/flight reaction and is typically replaced by the adult startle reflex by four months old. If a child experiences a retained Moro reflex beyond 4 months, he may become over sensitive and over reactive to sensory stimulus resulting in poor impulse control, sensory overload, anxiety and emotions and social immaturity. Some additional signs of a retained moro reflex are motion sickness, poor balance, poor coordination, easily distracted, unable to adapt well to change, and mood swings.
Rooting Reflex
The rooting reflex assists in the act of breastfeeding and is activated by stroking a baby’s cheek, causing her to turn and open her mouth. Retention of the rooting reflex beyond four months may result in difficulty with solid foods, poor articulation and thumb sucking.
Palmer Reflex
The palmer reflex is the automatic flexing of fingers to grab an object and should integrate by six months. If the palmer reflex is retained, a child may have difficulty with fine motor skills, stick out tongue while writing and exhibit messy handwriting.
Asymmetrical Tonic Neck Reflex
Asymmetrical tonic neck reflex (ATNR) is initiated when laying babies on their back and turning their head to one side. The arm and leg of the side they’re looking should extend while the opposite side bends. This reflex serves as a precursor to hand-eye coordination and should stop by six months. The purpose of the ATNR is to provide stimulation for developing muscle tone and the vestibular system whilst in the womb before birth.
The retained ATNR prevents a baby from developing certain physical cross pattern movements such as rolling over and later marching using alternate leg and arms. A retained ATNR is often thought to be associated with dyslexia and attention deficit disorder.
Spinal Galant Reflex
The spinal galant reflex happens when the skin along the side of an infant’s back is stroked, the infant will swing towards the side that was stroked. This reflex helps with the birthing process and should inhibit between three and nine months. If it persists, it may affect a child’s posture, coordination attention and ability to sit still. Retention of the spinal galant reflex is also associated with bedwetting.
Tonic Labyrinthine Reflex
The tonic labyrinthine reflex (TLR) is the basis for head management and helps prepare an infant for rolling over, creeping, crawling, standing and walking. This reflex initiates when you tilt an infant’s head backwards while placed on the back causing legs to stiffen, straighten and toes to point. Hands also become fisted and elbows bend. It should integrate gradually as other systems mature and disappear by 3 1/2 years old. If retained, the TLR can lead to poor muscle tone, tendency to walk on toes, motion sickness and poor balance.
Landau Reflex
The landau reflex assists with posture development and technically isn’t a primitive reflex as it isn’t present at birth. It is when a baby lifts his head up causing the entire trunk to flex and typically emerges at around 3 months of age. It is fully integrated by one year. If the landau reflex persists beyond this point, children may experience short term memory problems, poor motor development and low muscle tone.
Symmetrical Tonic Neck Reflex
Also known as the crawling reflex, symmetrical tonic neck reflex (STNR) is present briefly after birth and then reappears around six to nine months. This reflex helps the body divide in half at the midline to assist in crawling – as the head is brought towards chest, the arms bend and legs extend. It should disappear by 11 months. Developmental delays related to poor muscle tone, tendency to slump while sitting, and inability to sit still and concentrate can result if the STNR is retained.
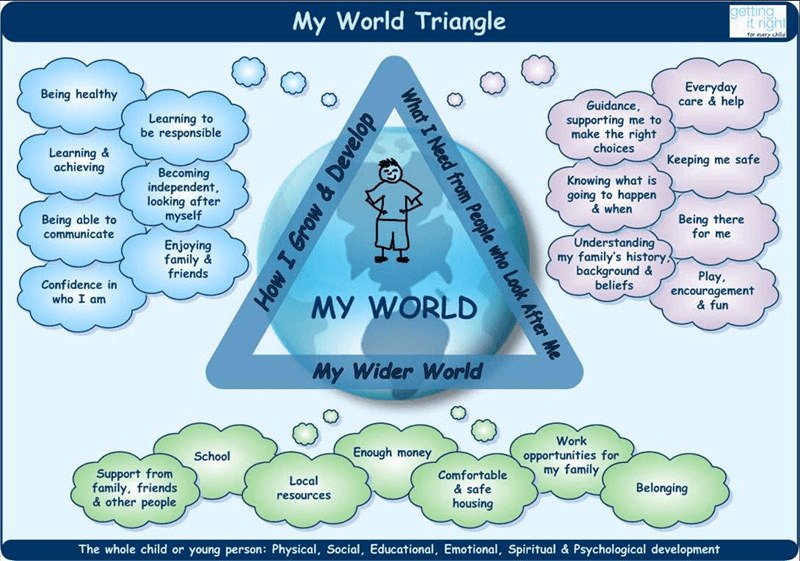
GIRFEC (Getting It Right For Every Child) introduced the My World Triangle which can be used when working with children or young people at every stage to think about their world and how the children grow and develop. My World Triangle promotes a holistic perspective of influence in a child's life and encourages practitioners and parents to think about their needs, risks and positive aspects of their lives.

Contact Us
Help your child reach his or her full potential. We can help. Get in touch to find out more.



About Us
The Learning Triangle is a dedicated space addressing learning, behavior, and sensory challenges rooted in neuro-motor and sensory immaturities. Our program gently integrates primitive reflexes, fostering holistic progress in academics, sports, and social settings.
Contact Us
Dublin clinic:
Amatsu Clinic, Unit 7, Sandyford Hall Centre, Dublin
D18 F438
Wexford clinic:
Amstelveen, Church Road, Bunclody,
Co. Wexford
Y21 AN22
Tel:
+353872903847
© 2023 The Learning Triangle
Website design done by student at ImpulseHub